
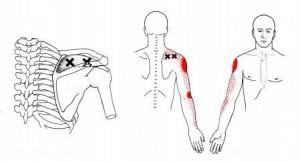
Last month I talked about trigger points and shoulder pain in the posterior rotator cuff (Infraspinatous and Teres Minor) along with their common referral patterns. Another common shoulder muscle to find active trigger points is the supraspinatous. Active trigger points in this muscles can refer pain to the deltoid and down the lateral aspect of the arm.
Check out the typical trigger points and referral patterns below:

Check out the video below for a demonstration of dry needling to the supraspinatous:
Case study:
Current patient of mine presents with lateral arm pain of 3 months duration. No known cause of injury but diagnosed with tricep injury/tear.
Pre-Treatment Testing
Selective Functional Movement Assessment (SFMA) dysfunctional non-painful patterns:
all cervical patterns (mobility dysfunction)
R shoulder medial rotation + extension T9 (mobility dysfunction) – Functional and non-painful (FN) to the L
Multi-Segmental (MS) rotation R (motor control deficit) – (FN) to the L.
SFMA dysfunctional painful patterns:
R shoulder lateral rotation + flexion (flexion limited to 140 degrees)
MS extension (R UE pain)
Special tests:
Hawkins + on the R
Passive shoulder IR 20 deg.
Palpation:
Tenderness with palpation of both trigger point in the supraspinatous with referral of pain down the lateral upper extremity to the wrist (pt indicates that is the pain he gets into the upper arm)
Treatment on Day 1 consisted of Functional Dry Needling to the supraspinatous (x2) with electrical stimulation followed by more superficial Graston technique to the R upper trap, supraspinatous, infraspinatous, and teres minor along with light strumming at the supraspinatous insertion. Corrective exercise consisted of 3pt. thoracic rotation (UE positioned in internal rotation – hand behind the back) with manual assist initially to hold/relax work until pt. was able to control the full available range.
Post-Treatment Testing
Functional Non-Painful patterns:
R shoulder medial rotation + extension (T7)
MS rotation B
SFMA dysfunctional non-painful patterns:
all cervical patterns (mobility)
SFMA dysfunctional painful patterns :
R shoulder lateral rotation + flexion (flexion improved to 160 degrees)
MS extension (R UE pain)
***both are still painful although intensity has decreased while motion has increased***
Special tests:
Hawkins + on the R but much less intense
Passive shoulder IR 50 deg.
Bottom Line
Trigger points with active referral patterns need to be treated right away, especially when they recreate the patient’s pain. In this case the patient’s pain decreased immediately along with a significant improvement in shoulder range of motion. This just confirms that this will be a critical area to continue to treat.
Joe Heiler PT, CSCS
Joe Heiler MSPT is the owner and content manager of SportsRehabExpert.com, a website dedicated to advancing the education of rehab and performance professionals. The site focuses on orthopedic and sports physical therapy topics through webinars, audio interviews, articles, manual therapy and exercise videos, and more.
Joe is also the owner of Elite Physical Therapy and Sports Performance in Traverse City, MI specializing in orthopedics and sports medicine, as well as athletic performance training. He is Graston Technique (GT) Certified as well as a GT Instructor, SFMA and FMS trained, and is passionate about a number of soft tissue and manual techniques including Trigger Point Dry Needling and manipulation.
Latest posts by Joe Heiler PT, CSCS (see all)
- The Bird Dog – A Core Stability Classic - April 4, 2016
- Trigger Points and Shoulder Pain – Part 2 - February 29, 2016
- Trigger Points and Shoulder Pain – Part I - January 19, 2016
- Core Stability vs Core Strength – Part II - April 1, 2009
- Core Stability vs Core Strength - March 1, 2009